When cells are implanted into the heart after a heart attack, the vast majority of them succumb to the hostile environment in the heart and die. Twenty-four hours after implantation there is a significant loss of cells (see Wu et al Circulation 2003 108:1302-1305). That fact that implanted bone marrow or fat-based stem cells benefit the heart despite their evanescence is a remarkable testimony to their healing power.
To mitigate this problem, stem cell scientists have used a variety of different strategies to increase the heartiness and survival of implanted stem cells. Two main strategies have emerged: preconditioning cells and genetically engineering cells. Both strategies increase the survival of implanted stem cells (see here, and here).
When it comes to genetically engineering stem cells, Lee and Julie Chao from the Medical University of South Carolina in Charleston, South Carolina have used endothelial progenitor cells (EPCs) from human umbilical cord blood to treat mice that had suffered heart attacks, except that these cells were genetically engineered to express “Tissue Kallikrein” or TK. TK is encoded by a gene called KLKB1, which is on chromosome 4 at region q34-35 (in human genetics, the long arm of a chromosome is the “q” arm and the small arm is the “p” or petite arm). TK is initially synthesized as an inactive precursor called prekallikrein. Prekallikrein must be clipped in order to be activated and the proteases (proteases are protein enzymes that cut other proteins into smaller fragment) that do so are either clotting factor XII, which plays a role in blood clotting, and PRCP, which is also known as Lysosomal Pro-X carboxypeptidase.
TK is a protease that degrades a larger protein called kininogen in two smaller peptides called bradykinin and kallidin, both of which are active signaling molecules. Bradykinin and kallidin cause relaxation of smooth muscles, thus lowering blood pressure, TK can also degrade plasminogen to form the active enzyme plasmin.
So why engineer EPCs to express TK? As it turns out, TK activates an internal protein in cells called Akt, and activated Akt causes cells to survive and prevents them from dying (see Krankel et al., Circulation Research 2008 103:1335-1343; Yao YY, et al., Cardiovascular Research 2008 80: 354-364; Yin H et a., J Biological Chem 2005 280: 8022-8030).
The first experiments were test tube experiments in which TK EPCs were incubated with cultured heart muscle cells to determine their ability to prevent cell death. When cultured heart muscle cells were exposed to hydrogen peroxide, they died left and right, but when they were incubated with the TK-EPCs and hydrogen peroxide, far fewer of them died.
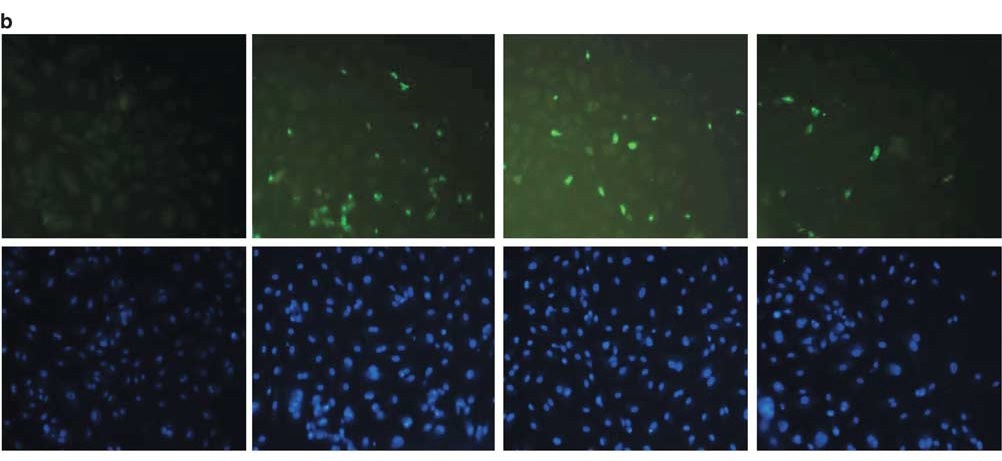
From left to right, normal cells, cell exposed to hydrogen peroxide, cells exposed to hydrogen peroxide plus the genes for TK, and finally, cells exposed to hydrogen peroxide and TK-EPCs.
When these cells were exposed to low levels of oxygen, a similar result was observed, expect that the cells co-incubated with TK-EPCs showed significantly less cell death.
When TK-EPCs were injected into the infarct border zones of the heart just after they had heart attacks, the results seven days after the heart attacks were striking. The heart function of the control mice was lousy to say the least. The heart walls had thinned, their ejection fractions were in the tank (~23%) and their echocardiograms were far from normal. However, the TK-EPC-injected mice had a relatively normal echocardiogram, thick heart wall, pretty good ejection fractions (52% and oppose to the 76% of mice that had never had a heart attack), and good heart function in general. Also, the size of the infarcts was reduced in those animals whose hearts had been injected with TK-EPCs.

There were two other bonuses to using TK-EPCs. First, as expected, the density of new blood vessels was substantially higher in hearts that received injections of TK-EPCs. Secondly, the TK-EPCs definitely survived better than their non-genetically engineered counterparts.

These results also confirm that TK works in heart muscle cells by activating the Akt protein inside the cells. This establishes that TK works through the Akt pathway.
Once again, we see that transplantation of stem cells after a heart attack can improve the function and structure of the heart after a heart attack. Indeed this strategy seems to work again and again. These experiments were done in mice and therefore, they must be successful in a larger animal, like a pig before they can be deemed efficacious and safe for use in human clinical trials. Even so, these results are hopeful.