When pluripotent stem cells are differentiated into photoreceptor cells, and then implanted into the retina at the back of the eye of a laboratory animal, they do not always survive. However, pre-treatment of those cells with an antiaging glycoprotein (AAGP), made by ProtoKinetix, causes those transplanted cells to be 300 times more viable than cells not treated with this protein according to a study recently accepted for publication.
AAGP was invented by Dr. Geraldine-Castelot-Deliencourt and developed in partnership with the Institute for Scientific Application (INSA) of France. For her work in this area Dr. Castelot-Deliencourt was honored with France’s highest award for scientific accomplishment, the Francinov Award, in 2006.
AAGP significantly improves the viable yield of stem cells transplanted in retinal tissue, according to experiments conducted at the University of British Columbia in the laboratory of Dr. Kevin Gregory-Evans.
AAGP seems to protect cells from inflammation-induced cell death. This is based on experiments in which cultured cells that were treated with AAGP were significantly more resistant to hydrogen peroxide, ultraviolet A (wavelengths of 320-400 nanometers), and ultraviolet C (shorter than 290 nm). In addition, when exposed to an inflammatory mediator, interleukin β (ILβ), AAGP exposure reduced COX-2 expression three-fold. COX-2 is an enzyme that is induced by the various stimuli that stimulate Inflammation. It is, therefore, an excellent read-out of the degree to which inflammation has been induced. The fact that AAGP prevented the induction of COX-2 shows that this protein can inhibit the induction of inflammation. These data suggest that AAGP™ may not just be usable in cell and organ storage but also in pharmacological treatments.
A presentation at the annual meeting of the Association for Research in Vision and Ophthalmology in Seattle, Washington has reported the safe transplantation of stem cells derived from a patient’s skin to the back of the eye in an effort to restore vision. The subject for this research project suffered from advanced wet age-related macular degeneration that did not respond to current standard treatments.
A small skin biopsy from the patient’s arm was collected and reprogrammed into induced pluripotent stem cells (iPSCs). The iPSCs were then differentiated into retinal pigmented epithelial (RPE) cells, which were transplanted into the patient’s eye. The transplanted cells survived without any adverse events for over a year and resulted in slightly, though significantly, improved vision.
iPSCs are adult cells that have been reprogrammed to an embryonic stem cell-like state, which can then be differentiated into any cell type found in the body.
Abstract Title: #3769: Transplantation of Autologous induced Pluripotent Stem Cell-Derived Retinal Pigment Epithelium Cell Sheets for Exudative Age Related Macular Degeneration: A Pilot Clinical Study by Yasuo Kurimoto and others from the laboratory of Masayo Takahashi’s laboratory at the RIKEN Center for Developmental Biology in Kobe, Japan.
Unfortunately, this clinical trial has been suspended because iPSCs made from other patients proved to possess too many genetic abnormalities. Therefore, Takahashi and her colleagues have decided that allogeneic iPSCs differentiated into RPEs will probably do a better job than the patient’s own skin cell-derived iPSCs.
Collaboration between scientists from mainland China, the University of California, San Diego School of Medicine and Shiley Eye Institute have developed a new, stem cell-based technique that permits remaining stem cells to regrow functional lenses after the diseased lens was removed. This treatment was initially tested in laboratory animals, but it has now been tested in a small human clinical trial. This procedure produced far fewer surgical complications than the current standard-of-care. The real boost is that this regenerative procedure resulted in regenerated lenses that had superior visual qualities in all 12 of the pediatric cataract patients who served as subjects for this clinical trial.
Kang Zhang, MD, PhD, chief of Ophthalmic Genetics, founding director of the Institute for Genomic Medicine and co-director of Biomaterials and Tissue Engineering at the Institute of Engineering in Medicine, both at UC San Diego School of Medicine, said: “An ultimate goal of stem cell research is to turn on the regenerative potential of one’s own stem cells for tissue and organ repair and disease therapy.” Zhang and his colleagues published their work in the journal Nature.
Cataracts are cloudiness over the lens of the eye that blurs vision. The lens consists mostly of water and protein. When the protein aggregates, it clouds the lens and reduces the light that reaches the retina. This clouding may become severe enough to cause blurred vision. Most age-related cataracts develop from protein clumpings. You do not have to be older to suffer from cataracts. Congenital cataracts occur at birth or shortly after birth. Scarring of the retina or prenatal damage to the eye can cause congenital cataracts. Congenital cataracts are a significant cause of blindness in children. Current treatment for congenital cataracts is limited by the age of the patient. Most pediatric patients require corrective eyewear after cataract surgery.
To address this medical need, Zhang and colleagues examined the regenerative potential of endogenous stem cells on the lens. Unlike other stem cell approaches that involve creating stem cells in the lab and introducing them back into the patient, Zhang decided to use stem cells that are already in place at the site of the injury to do the heavy lifting. In the human eye, lens epithelial stem cells or LECs generate replacement lens cells throughout a person’s life, even though their production declines with age.
Unfortunately, current cataract surgeries essentially remove LECs within the lens. Whatever cells might be left over produce disorganized regrowth in infants and no useful vision. Zhang and his colleagues first confirmed that LECs had regenerative potential. To confirm this, they used laboratory animals. With that knowledge in hand, Zhang and his collaborators devised a novel, minimally invasive surgical procedure that removes the cloudy lens, but manages to maintain the integrity of the membrane that gives the lens its required shape (the lens capsule). With the lens capsule in place, the LECs were activated to replace the missing lens.
Once again, Zhang and his team ensured that their technique worked in animals before they ever tried it on a human patient. Animals with cataracts whose lenses were extirpated, but whose lens capsules were left intact, regenerated new lenses that were devoid of cataracts and provided excellent sight. With their technique honed and ready, Zhang and others tested their procedure on very young human infants in a small human trial. They discovered that their new surgical technique allowed pre-existing LECs to efficiently regenerate functional lenses. In particular, the human trial involved 12 infants under the age of 2 treated with the new method developed by Zhang and others, and 25 similar infants receiving current standard surgical care.
The results were stark: the control group experienced a higher incidence of post-surgery inflammation, early-onset ocular hypertension and increased lens clouding, but those infants who received Zhang’s new procedure showed fewer complications and faster healing. After three months, the 12 infants who underwent the new procedure had a clear, regenerated biconvex lens in all of their eyes.
“The success of this work represents a new approach in how new human tissue or organ can be regenerated and human disease can be treated, and may have a broad impact on regenerative therapies by harnessing the regenerative power of our own body,” said Zhang.
Zhang indicated that he and his colleagues are now looking to apply what they learned in this project to tackling the issue of age-related cataracts. Age-related cataracts are the leading cause of blindness in the world. Over 20 million Americans suffer from cataracts, and more than 4 million surgeries are performed annually to replace the clouded lens with an artificial plastic lens (intraocular lens).
Despite technical advances, a large portion of patients undergoing surgery are left with suboptimal vision post-surgery and are dependent upon corrective eyewear for driving a car and/or reading a book. “We believe that our new approach will result in a paradigm shift in cataract surgery and may offer patients a safer and better treatment option in the future,” said an optimistic Zhang.
Retinal degenerations are the leading cause of blindness and fixing a defective retina is not an easy task.
Fortunately, a model system in nonhuman primates that has been used to test retinal replacement with stem cell-derived retinal cells has seen some success. In several experiment in small animals, retinal transplantations helped blind animals regain their sight. However, small laboratory rodents are not terribly good model systems for human eye problems.
To address the clinical relevancy of this transplantation system, Shirai and colleagues confirmed in rats and in macaques that transplantion of human embryonic stem cell (hESC)–derived retinas integrate into the already-existing retina and develop as fully mature retinal grafts.
In this paper, Shirai and others established the developmental stage at which embryonic stem cell-derived retinal cells could integrate into the retina and replace damaged cells. By transplanting cells into nude rats that do not have the ability to reject transplanted tissue, they refined their cell-based technique to heal damaged retinas. Then they took their refined technique into macques to treat two newly established monkey models of retinal degeneration.
In the first model system, Shirai et al. exposed one group monkeys to retina-damaging chemicals, and the other group had their retinas damaged by lasers. In both cases, the result was photoreceptor degeneration. Anywhere from 46 to 109 days after injury, the human embryonic stem cell-derived retinal sheets were implanted into the damaged retinas.
The retinal grafts integrated into the primate eyes and continued to differentiate into cone and rod cells, which are the two types of photoreceptor cells in the retina. Functional studies are still being conducted, but if vision can be improved, but these new macaque models confirm the clinical potential of stem cell–derived grafts for retinal blindness that results from photoreceptor degeneration.
See H. Shirai et al., Transplantation of human embryonic stem cell-derived retinal tissue in two primate models of retinal degeneration. Proc. Natl. Acad. Sci. U.S.A.113, E81–E90 (2015).
Masayo Takahashi, an ophthalmologist at the RIKEN Center for Developmental Biology (CDB) in Kobe, Japan, has pioneered the use of induced pluripotent stem cells (iPSCs) to treat patients with degenerative retinal diseases.
Takahashi isolated skin cells from her patients, and then had them reprogrammed into iPSCs in the laboratory through a combination of genetic engineering and cell culture techniques. These iPSCs have many similarities with embryonic stem cells, including pluripotency, which is the potential to differentiate into any adult cell type.
Once induced pluripotent stem cell lines were established from her patient’s skin cells, they had their genomes sequenced for safety purposes, and then differentiated into retinal pigmented epithelial (RPE) cells. RPE cells lie beneath the neural retina and support the photoreceptors that respond to light. When the RPE cells die off, the photoreceptors also begin to die.
Takahashi watched the transplantation of the RPE cells that she had grown in the laboratory into the back of a woman’s damaged retina. This transplant would constitute the first test of the therapeutic potential of iPSCs in people. Takahashi described the transplant as “like a sacred hour.”
Takahashi has collaborated with Shinya Yamanaka, the discoverer of iPSC technology. She devised ways to convert the iPS cells into sheets of RPE cells. She then tested the resulting cells in mice and monkeys, jumped the various regulatory loops, recruited patients for her clinical trial, and practiced growing cells from those patients. Finally, she was ready to try the transplants in people with a common condition called age-related macular degeneration, in which wayward blood vessels destroy photoreceptors and vision. The transplants are meant to cover the retina, patch up the epithelial layer and support the remaining photoreceptors. Watching the procedure, “I could feel the tension of the surgeon,” Takahashi said.
This transplant surgery occurred approximately a year ago. Some new data on this patient is available.
As of 6 months after the transplant, the procedure appears to be safe. The one-year safety report should appear soon. Prior to the transplant, the patient was a series of 18 anti-vascular endothelial growth factor (anti-VEGF) ocular injections for both eyes to cope with the constant recurrence of the disease. However, data presented by Dr. Takahashi showed that the patient had subretinal fibrotic tissue removed during the transplant surgery in order to make room for the RPE cells. Once the RPE cells were implanted, the patient experienced no recurrence of neovascularization at the 6-month point. This is significant because she has not had any other anti-VEGF injections since the transplant. Her visual acuity was stabilized and there have been no safety related concerns to date.
I must grant that this is only one patient, but so far, these results look, at least hopeful. Hopefully other patients will be treated in this trial, and hopefully, they will experience the same success that the first patient is enjoying. We also hope and pray that the first patient will continue to experience relief from her retinal degeneration.
As to the treatment of the second patient of this trial, Takahashi has hit a snag. Some mutations were detected in the iPS cell-derived RPE cells prepared for the second patient. No one knows if these mutations make these cells dangerous to implant. Regulatory guidelines, at this point, are also no help. Apparently, the cells have three single-nucleotide change and three copy-number changes that are present in the RPE cells that were not detectable in the patient’s original skin fibroblasts. The copy-number changes were, in all cases, single-gene deletions. One of the single-nucleotide changes is listed in a database of cancer somatic mutations, but only linked to a single cancer. Further evaluation of these mutations shows that they were not in “driver genes for tumor formation,” according to Dr. Takahashi.
Tumorigenicity tests in laboratory animals has established that the RPE cells are safe. Remember that the presence of a mutation does not necessarily mean that these RPE cells can be tumorigenic.
However, Takahashi has still decided to not transplant these cells into the second patients. Part of the reason is caution, but the other reason is compliance with new Japanese law on Regenerative Medicine, which became effective after iPS trial was begun. This law, however, does not specify how safe a cell line has to be before it can be transplanted into a patient.
RIKEN’s decision to halt the trial is probably a good idea. After all, this is the first trial with iPSCs and it is important to get it right. Even though the RPE cells were widely thought to be safe to use, Takahashi decided not to implant another patient with RPEs derived from their own cells. Instead, they decided to use RPEs made from donated iPSC lines. Therefore, Takahashi is in discussions government officials to determine how this change of focus for the trial affects their compliance with Japanese law.
Frankly, this might be a very savvy move on Takahashi’s part. As Peter Karagiannis, a spokesperson for the Center for iPS Cell Research and Application, noted: “As of now, autologous would not be a feasible way of providing wide-level clinical therapy. At the experimental level it’s fine, but if it’s going to be mass-produced or industrialized, it has to be allogeneic.”
Therefore, the RIKEN institute is moving forward with allogeneic iPSC-derived RPEs. RIKEN will work in collaboration with the Center for iPS Cell Research and Application (CiRA) in Kyoto, Japan, which has several well characterized, partially-matched lines whose safety profiles have been established by strict, rigorous safety testing methods. However, immunological rejection remains a concern, even if these cells are transplanted into an isolated tissue like the eye where to immune system typically is not allowed. The simple fact is that no one knows if the cells will be rejected until they are used in the trial.
An additional concern is that CiRA has not typed its cells for minor histocompatibility antigens, which can cause T cell–mediated transplant rejection.
Nevertheless, Takahashi and her team deserve a good deal of credit for their work and vigilance.
If we take tissue samples from the mouth and grow them in the laboratory and manipulate them, we might be able to cure the blind. Blind people who suffer from stem cell deficiency in the cornea might be able to see again by using stem cells isolated from the mouth. Furthermore, this treatment might not only restore vision, but it might also ameliorate pain in the cornea.
Ophthalmologist Tor Paaske Utheim has conducted research for over ten years on how to cure certain types of blindness by using stem cells harvested from tissue obtained from different parts of the body. He then transplants this cultured tissue into the damaged eye, and patients who suffer from blindness as a result of corneal stem cell deficiencies can regain their sight. Recently, Utheim’s research has utilized stem cells from the mouth to grow new corneal tissue, and has also tried to design optimal methods to store and transport this tissue to treat patients.
Utheim is the head of a research group at the Faculty of Dentistry at the University of Oslo (UiO) and the Department of Medical Biochemistry at Oslo University Hospital.
Using cells extracted from the mucous membrane lining the inside of the mouth (the oral mucosa) can restore vision is new to most people. Only ten years ago, this was considered impossible, but results confirm the potential of this method. Twenty clinical studies from various countries have, to date, shown good results, according to Utheim. These clinical trials, however, have only applied these cells to a group of diseases caused by stem cell deficiency in the cornea.
Utheim and his colleagues hope to treat patients with eye injuries caused by so-called limbal stem cell deficiencies. This disorder can be caused by such things as UV radiation, chemical burns, serious infections like trachoma, and various other diseases, some of which are heritable. The number of people worldwide affected by limbal stem cell deficiency is unknown, but in India alone there is an estimated 1.5 million. This disorder most often affects people living in developing countries.
Stem cells that are found at the outer edge of the cornea help to keep the surface of the cornea even and clear. In limbal stem cell deficiencies, the stem cells have been damaged, and they cannot renew the cornea’s outermost layer. Instead, other cells grow over the cornea, which clouds the cornea. The cornea can become fully or partially covered, explains Utheim, which leads to impaired vision or blindness.
The stem cells are localized in the periphery of the cornea; an area known as the limbus. These limbal stem cells renew the outermost layer of the cornea. Illustration: Amer Sehic, OD/UiO.
Others suffer from severe pain as well. When one patient was interviewed by Norwegian national broadcaster NRK about his limbal stem cell deficiency, he responded: “I don’t know what’s worse: the pain, or losing my sight.”
Utheim explained that when stem cells do not work properly, ulcers can develop in the cornea, which exposed nerve fibers. Since the number of nerve fibers is far higher in the cornea than for example in the skin, it is not surprising that some patients experience severe pain.
Eyes that suffer mildly from limbal stem cell deficiency. The stem cells stall and other cells grow over the cornea. The window of the eye, normally clear and transparent, is thus blurred, leading to reduced vision. Photo: Dr. Takahiro Nakamura, Department of Ophthalmology/Kyoto Prefectural University of Medicine.
A breakthrough within the field occurred about ten years ago when Japanese researchers showed that cells from the oral mucosa could be used to replace limbal stem cells in patients with limbal stem cell deficiency. Although it had been possible since the late 1990s to cure the disorder using cultured stem cells. The available treatment relied on the patient having a healthy eye from which to collect cells.
Further developments made it possible to harvest cells from a relative or deceased individual, but using limbal stem cells from other patients required the use of strong immunosuppressive drugs for the patients, which could cause serious side effects.
A milestone seemed to be reached when it became possible to use a patient’s own cells to treat blindness in both eyes without the need for immunosuppressive drugs. Strangely, this makes some sense because there are similarities between the oral mucosae and the surface of the eye (see Utheim TP. Stem Cells. 2015;33:1685-1695). Originally, using mouth mucosal cells to treat the eye required that the laboratory where the cells are cultured and the clinic where the patients are treated be quite close together. Because there were no protocols for storing extracted oral mucosal cells so that they can be easily kept and transported. This has made the treatment virtually inaccessible to many of the patients who need it the most, namely those in developing countries. However, this may be about to change.
Utheim’s research group is now on the brink of a development that will make it possible to cure both severe pain and blindness in patients who are spread over a larger geographical area than before (see Islam R, et al. PLoS One. 2015;10:e0128306.). “Today, cells from the mouth are cultured for use in the treatment of blindness in only a few specialized centers in the world. By identifying the optimal conditions for storing and transporting the cultured tissue, we would allow for the treatment to be made available worldwide, and not just close to the cell culture centers,” said Rakibul Islam, who is a PhD candidate in the Department of Oral Biology at the Faculty of Dentistry.
Islam is collaborating with Harvard Medical School to introduce this method of treating blindness to clinics around the world. Islam’s findings could also help improve treatment outcomes. “Being able to store the cultured tissue in a small sealed container for a week increases the technique’s flexibility significantly. It makes it easier to plan the operation and allows for quality assurance through microbiological testing of the tissue before transplantation,” Islam explained.
One of the things that Islam and his colleagues have discovered is the specific temperature range at which cells from the mouth should ideally be stored at after culture. Islam has shown that cultured mouth stem cells retain their quintessential properties best between 12 and 16 degrees Celsius (See Dolgin, Elie. Nature Biotechnolgy, 2015;33:224-225.).
During a brief stint at Harvard University, Islam also examined which areas of the mouth are best suited to use in regenerative medicine. In other words, Islam and his colleagues wanted to know which parts of the mouth contain cell layers that regenerate the fastest. Islam explained this using this example: “If you burn any part of your mouth on hot coffee, it heals so quickly that by the next morning you have forgotten about it. This is because the oral mucosa contains cells that multiply quickly. We wanted to investigate whether there were regional differences in the mouth that we could exploit for the treatment of limbal stem cell deficiency.”
Islam continued, “Our results show that the location from which the mucosal tissue is harvested has a striking impact on the quality of the cultured tissue.”
The results from this particular study have not yet been published.
This research can potentially give hope to the many blind that live far away from centralized cell culture laboratories. In work by Utheim in 2010, in collaboration with the ophthalmologist Sten Ræder, he developed storage technology for cultured stem cells that enables the cultured tissue to be transported in a small custom-made plastic container. Tissue from stem cells is thus freed from expensive and bulky laboratory equipment and provides a whole new level of flexibility.
Utheim said “The sample of cells from the mouth can be sent by air over long distances to specialist laboratories with first-class equipment and expertise. After a couple of weeks of laboratory cultivation, the sender may receive the tissue back ready for use. An ophthalmologist could then transplant the stem cells onto the patient’s eye.”
However, the container was just one step in the right direction: “Now we have identified those areas of the mouth that may be best suited for regenerative medicine, and developed a method for storing and transporting tissue from centralized, highly specialized tissue culture centers to clinics worldwide. Our findings are helping to simplify and streamline the clinical procedures, and to make the treatment far more accessible than it is today,” said Islam, who admitted that the transport potential of the project has been integral to his own enthusiasm. He continued, “Although the scientific and technical aspects of our project are very exciting, it has been especially motivating to think of the possibilities this storage technology brings to treating blindness in all parts of the world, including my homeland Bangladesh.”
A central laboratory for the growth of stem cells already exists in Italy. In fact, earlier this year the European Medicines Agency approved the procedure for the cultivation of stem cells from the cornea in EU laboratories. This is the first stem cell therapy to be approved by the European Medicines Agency, according to the journal Nature Biotechnology. Utheim described the approval as an important step towards the implementation of stem cell technology over larger geographical areas. To date, almost 250 people with limbal stem cell deficiency have undergone treatment involving transplantation of stem cells grown from their own mouth cells. “This provides a good basis for judging the success of the treatment” Utheim says.
He has recently published an article in the journal Stem Cells on the inherent potential of cells from the mouth to regenerative medicine. Roughly three out of four treatments are described as successful.
Stem cell transplantation is a promising potential treatment for retinal degenerative diseases. Because retinal degeneration often leads to blindness, stem cells might be one of the up-and-coming tools in the battle against blindness.
The laboratory of Shaomei Wang (Cedars-Sinai Medical Center, Los Angeles) have assessed the effectiveness of stem cell-based therapeutic strategies using the Royal College of Surgeons (RCS) rat model, which mimics the disease progression of age-related macular degeneration (AMD). In RCS mice, the retinal pigment epithelium or RPE degenerates and is disrupted, which leads to the death of photoreceptors (Mullen RJ and LaVail MM Inherited retinal dystrophy: primary defect in pigment epithelium determined with experimental rat chimeras. Science 1976;192:799-801). The work by Wang and his colleagues has shown that human cortical-derived neural progenitor cells (hNPCctx) could dramatically rescue vision in the RCS rat (see Wang S, and others, Investigative ophthalmology & visual science 2008;49:3201-3206; Gamm DM, and others, Wang S, Lu B, et al. PLoS One 2007;2:e338). Unfortunately, the fetal origin of these cells presents an obstacle, because such cells are not readily available and come from aborted fetuses.
To overcome such obstacles, Wang and his colleagues assessed the ability of a stable neural progenitor cell line (iNPCs) derived from induced pluripotent stem cells (iPSCs) to preserve vision after sub-retinal injection into RCS rats (Sareen D, and others, J Comp Neurol 2014;522:2707-2728). A report in the journal Stem Cells by Wang and others establishes that iNPC injection leads to the reversal of AMD-related symptoms, the preservation of visual function, and may represent a patient-specific therapeutic option (Tsai Y, and others, Stem Cells 2015;33:2537-2549).
Wang and his others showed that an iNSC-treated eye scored higher in all functional tests used (optokinetic response (OKR), electroretinography (ERG), and luminance threshold responses (LTR)), compared to an untreated eye, in RCS mice at 150 days post-transplant. This improvement nicely correlates with the improved protection of photoreceptors in iNPC-treated eyes, which presented with normal cone morphology and the reversal of disease-associated changes throughout the retina.
So how do iNPCs help preserve the photoreceptors and visual function? Wang and his team found that iNPCs survived up to 130 days in RCS retinas, which when normalized to lifespan, represents around 16 years in humans. Additionally, they discovered that iNPCs were able to migrate to an area between the retinal pigment epithelial and photoreceptor layers. This allows the injection of cells into non-affected neighboring regions of the retina, which will not to worsen any compromised retinal components. iNPCs did, however, continue to express NSC/NPC markers and did not mature neural/retinal markers, suggesting that grafted-iNPCs remained phenotypically uncommitted progenitor cells and did not differentiate towards a retinal phenotype.
Further investigations found that iNPC-treatment reduced levels of toxic undigested bits of the photoreceptor cell membranes. Accumulation of these photoreceptor outer segments (POS) cause the photoreceptors to die off. Typically, the RPE cells goggle up these toxic membrane bits, degrade them, and recycle their components for the photoreceptors. The fact that these POS bits were not accumulating in the retinas of RCS mice suggested to Wang and his colleagues that the grafted-iNPCs restored POS degradation in RCS rats. They subsequently found that iNPCs expressed phagocytosis-related genes and could gobble up and degrade POS in culture. They extended these findings in living creatures by identifying the different stages of POS digestion and even viewed engulfed membranous discs inside the cytoplasm of iNPCs.
Overall, iNPC injection appears to be a safe and effective long-term treatment for Acute Macular Degeneration in the RCS rat preclinical model, and holds great promise for the translation into a patient-specific treatment for the preservation of existing retinal structure and vision during the early stages of AMD in humans. Wang noted that iNPC treatment in this model occurred at later stages of degeneration, which represents a more clinical relevant stage. However, an unstudied possibility is restoring phagocytosis by iNPCs to treat loss of visual acuity early on in the course of the disease.
Induced pluripotent stem cell (iPSC) technology has raised the possibility that patient-specific pluripotent stem cells may become a renewable source of a patient’s own cells for regenerative therapy without the concern of immune rejection. However, the immunogenicity of autologous human iPSC (hiPSC)-derived cells is not well understood.
Using a humanized mouse model (denoted Hu-mice) with a functional human immune system, Yang Xu and his colleagues from UC San Diego has shown that most teratomas or tumors formed by human iPSCs were readily recognized by immune cells and rejected. However, when these human iPSCs were differentiated into smooth muscle cells or retinal pigmented epithelial cells, the results were rather different. Human iPSC-derived smooth muscle cells appear to be highly immunogenic, but human iPSC-derived retinal pigment epithelial (RPE) cells are tolerated by the immune system, even when transplanted outside the eye.
When Xu and others examined these results more closely, they discovered that this differential immunogenicity is due to the abnormal expression of cell surface proteins in hiPSC-derived Smooth Muscle Cells, but not in hiPSC-derived RPEs.
These findings support the feasibility of developing hiPSC-derived RPEs for treating macular degeneration. They also show that iPSC lines must be individually screened to determine if their derivatives are recognized by the patient’s immune system as foreign.
When a mouse sees an owl, it scurries for cover as fast as it can to escape the back-breaking talons of the swooping owl. If the mouse has defective vision and cannot properly see the owl, then the mouse is simply doomed. So ingrained is this escape response into the psyche of mice, that simply showing laboratory mice a video of a swooping owl will send them off into various directions for safety. Consequently, vision scientists can use this behavior to test treatments of blindness.
Rob Lucas of the University of Manchester, UK and his colleagues have played videos of swooping owls to normal and blind laboratory mice, and to blind mice that were treated with an experimental treatment for blindness. Lucas and others showed the owl video to mice that were so blind that they did not respond to the video. Then after giving these blind mice a treatment for blindness, those same mice were shown the same owl video, and they reacted as though they could see the swooping owl just fine. As Lucas explained: “You could say they were trying to escape, but we don’t know for sure. What we can say is that they react to the owl in the same way as sighted mice, whereas the untreated mice didn’t do anything.”
This best evidence acquired by Lucas and others to date that injecting the gene for a pigment that detects light into the eyes of blind mice can help them see again.
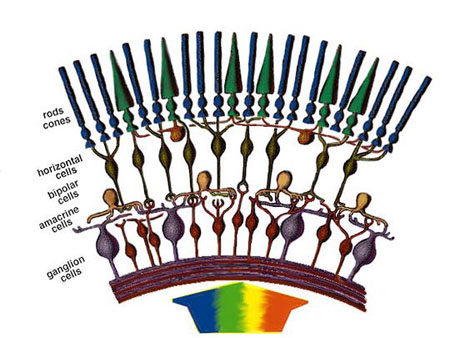
The gene therapy used by Lucas and others is meant to treat those types of blindness that are caused by damaged or missing photoreceptor, which are the cells in the neural retina that detect light. There are two types of photoreceptors in the retina: rods and cones. Rods and cones contain a pigment known as an “opsin,” which allows them to respond to light. Opsin genes encode proteins that contain a vitamin A-based cofactor that helps it respond to light. The amino acid sequence of each opsin gene allows it to specifically respond to a range of frequencies of light. Different types of cones express specific opsins that allow them to specialize in the colors they can detect. Mutations in the opsin genes can cause blindness, and Lucas and his colleagues are interested in replacing the defective opsin genes in the retinas of laboratory mice. The majority of gene therapy experiments to treat blindness to date have concentrated on replacing faulty genes in rarer, specific forms of inherited blindness, such as
When a mouse sees an owl, it scurries for cover as fast as it can to escape the back-breaking talons of the swooping owl. If the mouse has defective vision and cannot properly see the owl, then the mouse is simply doomed. So ingrained is this escape response into the psyche of mice, that simply showing laboratory mice a video of a swooping owl will send them off into various directions for safety. Consequently, vision scientists can use this behavior to test treatments of blindness.
Rob Lucas of the University of Manchester, UK and his colleagues have played videos of swooping owls to normal and blind laboratory mice, and to blind mice that were treated with an experimental treatment for blindness. Lucas and others showed the owl video to mice that were so blind that they did not respond to the video. Then after giving these blind mice a treatment for blindness, those same mice were shown the same owl video, and they reacted as though they could see the swooping owl just fine. As Lucas explained: “You could say they were trying to escape, but we don’t know for sure. What we can say is that they react to the owl in the same way as sighted mice, whereas the untreated mice didn’t do anything.”
This best evidence acquired by Lucas and others to date that injecting the gene for a pigment that detects light into the eyes of blind mice can help them see again.
The gene therapy used by Lucas and others is meant to treat those types of blindness that are caused by damaged or missing photoreceptor, which are the cells in the neural retina that detect light. There are two types of photoreceptors in the retina: rods and cones. Rods and cones contain a pigment known as an “opsin,” which allows them to respond to light. Opsin genes encode proteins that contain a vitamin A-based cofactor that helps it respond to light. The amino acid sequence of each opsin gene allows it to specifically respond to a range of frequencies of light. Different types of cones express specific opsins that allow them to specialize in the colors they can detect. Mutations in the opsin genes can cause blindness, and Lucas and his colleagues are interested in replacing the defective opsin genes in the retinas of laboratory mice. The majority of gene therapy experiments to treat blindness to date have concentrated on replacing faulty genes in rarer, specific forms of inherited blindness, such as Leber congenital amaurosis.
Structures of opsins and of the chromophore retinal. (a) A model of the secondary structure of bovine rhodopsin. Amino-acid residues that are highly conserved in the whole opsin family are shown with a gray background. The retinal-binding site (K296) and the counter ion position (E113) are marked with bold circles, as is E181, the counter ion in opsins other than the vertebrate visual and non-visual ones. C110 and C187 form a disulfide bond. (b) The chemical structures of the 11-cis and all-trans forms of retinal. (c) The crystal structure of bovine rhodopsin (Protein DataBank ID: 1U19 [PDB:1U19]). The chromophore 11-cis-retinal, K296 and E113 are shown in stick representation in the ringed area. (d) The structure of the Schiff base linkage formed by retinal within the bovine opsin, together with the counter ion that stabilizes it. Taken from Terakita A, The opsins. Genome Biol 2005; 6(5):213.The new treatment strategy employed by Lucas and others seek to enable other cells that lie just above the photoreceptors to capture light. Rod and cone cells normally detect light and convert it into an electrochemical signal that is sent to bipolar and then ganglion cells above them, which processing these signals and send them to the brain. By engineering bipolar or even ganglion cells to produce their own light-detecting pigment, they can to some extent compensate for the lost receptors, although the resolution of the vision is poor.
Lucas and others used the human gene for rhodopsin, the pigment used by rod cells to detect light and hooked this gene to a genetic “switch” that would only turn on the gene inside ganglion and bipolar cells. Then they inserted this DNA into a virus that infected the retinal cells of mice whose rods and cones had been destroyed.
After treatment, Lucas and his colleagues found that the mice could distinguish objects by their size quite well, but not as well as sighted mice. “The treated mice could discriminate black and white bars, but only ones that were 10 times thicker than what sighted mice could see,” says Lucas.
In earlier attempts, mice could only tell objects apart under extremely bright light. Therefore, this new finding is crucial. “Our mice could respond in ordinary light, the equivalent of looking at a computer monitor under ordinary office lighting,” says Lucas.
This is also the first time a human gene has been tested this way. The virus they used to deliver the gene therapy to mouse retinal cells has already been approved for use in humans, and Lucas says he hopes to begin trials of a human treatment in about five years.
“This is the most effective example yet of the use of genetic therapy to treat advanced retinal degeneration,” says Robin Ali, whose team at University College London has given gene therapy treatments of people with Leber congenital amaurosis.
But Robert Lanza, chief medical officer at Ocata Therapeutics in Marlborough, Massachusetts, warns that we don’t yet know how long the beneficial effects of the new treatment might last, since it seems that the sight in people with Leber congenital amaurosis who were treated with gene therapy between one and three years ago has begun to wane.
See Current Biology DOI: 10.1016/j.cub.2015.07.029.
A halt has been called to a pioneering stem cell clinical trial after genetic mutations were detected in the cells derived from one of the trial participants; cells that were to be used to treat the patient.
What makes this trial so unique is that it is the first to investigate if cells derived from induced pluripotent stem (iPS) cells can be used to treat disease. iPS cells are made from mature, adult cells that have been genetically engineered to transiently express four genes (Oct-4, Soc-2, Klf-4, and c-Myc), and then cultured in the laboratory in embryonic stem cell-type medium. This treatment kills many of the cells, but a fraction of them are developmentally regressed into a pluripotent stem-cell-like state. From this pluripotent state, the cells can be differentiated into almost any other type of cell in the body. Such differentiated cells can them be transplanted back into the body of the patient to replace diseased, dying cells.
In this trial, skin cells from trial participants were reprogrammed into iPS cells, which were then differentiated into retinal cells. Transplantation of these retinal cells could potentially interrupt or, perhaps even reverse, the damage caused by a disease called age-related macular degeneration, which leads to loss of vision and, potentially, blindness. The first patient in the trial, a 70-year-old woman, was treated in September, 2014, and is reportedly in good health.
Treatment of the second patient, however, has hit a snag. “A mutation was found in the cells before transplantation into the second patient, and this is something we took into account when we made the decision to suspend the study for the time being,” says trial leader Masayo Takahashi of the Riken Center for Developmental Biology in Kobe, Japan.
Analyses of the iPS cells made from skin cells taken from the second patient revealed six mutations. Three of these mutations consisted of deletion of particular genes, and the other three consisted of changes to genes, including one in an oncogene (a gene with the potential to cause cancer), although this one is linked with a low risk. The mutations were not detectable in the original skin cells, which suggests that they occurred as a result of the iPS-cell procedure. However, other work has shown that low-frequency mutations in the initial cells that are difficult to detect can become amplified in iPS cells derived from that cell population.
“Either they were there at undetectable levels in the skin cells, or they were caused by the iPS cell induction process,” says Shinya Yamanaka of Kyoto University in Japan, one of the scientists who developed the iPS cell reprogramming technique. “However, the risk of carcinogenesis was considered low.”
Other factors that caused the trial to be halted are regulatory changes in Japan. Takahashi told the magazine New Scientist that the law now stipulates that in Japan only certain institutions can run stem-cell trials. Once the team has worked out how to accommodate these changes, they hope to resume work and test five more people using healthy, mutation-free skin cells from younger people.
“I think it’s an easily fixable problem if they go this route,” says Robert Lanza, chief scientist at Ocata Therapeutics in Marlborough, Massachusetts, which is also developing stem-cell therapies for age-related blindness.
Regardless, the discovery of mutations that could be related to the process by which iPS-cells are derived is troubling, and is a concern that stem cell scientists have had since iPS cells were first discovered. One of the benefits of stem-cell therapies is that the cells can multiply rapidly, which is also a characteristic shared by cancer cells.
But that similarity doesn’t necessarily mean cancer will develop. “It’s important to understand that even mutations in oncogenes don’t guarantee that cancer will result,” says Jeanne Loring of the Scripps Research Institute in La Jolla, California.
“It will be important to determine the source of the mutation before jumping to conclusions that reprogramming cells will always carry this sort of risk,” says Mike Cheetham of the Institute of Ophthalmology at University College London. “It will be important to determine the source of the mutation before jumping to conclusions”
Scientists at the University of Pittsburgh have found a new way to treat corneal blindness, which affects millions of people around the world.
James Funderburgh and his colleagues at the University of Pittsburgh School of Medicine showed that stem cells isolated from the dental pulp of extracted wisdom teeth can be differentiated into specialized cells that can maintain the health and integrity of corneas and rid them of the scars caused by illness or injury that compromise the ability to see clearly. These cells can be safely injected into the corneas of mice.
According to Funderburgh, who is a professor of ophthalmology, this new approach can replace damaged corneal eye tissue with tissue made from the patient’s own cells rather than cells from a donor. Such a procedure circumvents the problems of immunological rejection that dog the reconstruction of corneal tissue with cells from donors. Furthermore, donor corneas are in short supply in certain parts of the world (e.g., Africa and Asia).
“Our work is promising because using the patient’s own cells for treatment could help avoid these problems,” said Dr. Funderburgh, who is the senior author of a new paper describing the research, in a written statement.
A post-doctoral research fellow in Dr. Funderburgh’s laboratory, Dr. Fatima Syed-Picard, took cells from the pulp of extracted wisdom teeth and chemically processed them to differentiate them into specialized corneal cells. Then Syed-Picard and others injected these “keratocytes” into the corneas of healthy mice. Once in the eyes of laboratory mice, the tooth pulp-derived cells integrated with the existing tissue with no sign of rejection even after several weeks.
Could such a treatment work in human patients? “We are thinking that in the future people may ‘bank’ their extracted wisdom teeth or the cells from those teeth,” Funderburgh told The Huffington Post in an email. “For someone who did not do that it is possible to extract dental pulp with a root canal procedure, but this is still hypothetical. In the worst-case scenario, someone might consider having a tooth extracted to provide cells for this procedure.”
Last year more than 70,000 corneal transplants were performed in the U.S., According to Kevin Corcoran, president and CEO of the Washington, D.C.-based Eye Bank Association of America (EBAA), there were more than 70,000 corneal transplants performed in the US alone.
“There’s a lot of exciting research being done in the area of [corneal] transplant, and EBAA is interested in any outcome that can help restore sight to the blind or visually impaired,” said Corcoran, who was unfamiliar with the Pitt research.
Dr. Syed-Picard stressed that this research is still in the formative stages and the results are preliminary, and added that it would probably take a few years before human testing could begin. The next step, she said, would be to conduct a similar set of experiments in rabbits.
The EMA, which is short for the European Medicines Agency, has recommended approval for a treatment called Holoclar. Holoclar is the first therapy product that contains stem cells to be recommended for approval in the European Union (EU). Holoclar is being marketed as a treatment for moderate to severe limbal stem cell deficiency (LSCD) due to physical or chemical burns to the eye in adults. In fact, Holoclar is the first medicine recommended for LSCD, a condition that can result in blindness.
Holoclar can be transplanted into the eye after removal of the corneal epithelium (the outer layer of the cornea). Holoclar is made from a biopsy taken from a small, undamaged area of the patient’s cornea. These limbal stem cells are then grown in the laboratory using cell culture techniques. Holoclar is a potential alternative to transplantation for replacing altered corneal epithelium. Clnical trials with Holoclar have been shown to increase the chances of a successful corneal transplant where the injury has caused extensive eye damage. Holoclar is produced by Chiesi, a pharmaceutical company based in Parma, Italy.
The recommendation to approve Holoclar was made by the EMA’s Committee for Medicinal Products for Human Use (CHMP). CHMP made their recommendation on basis of the benefits of Holoclar, which are its ability to repair the damaged ocular surface, to improve or resolve symptoms of pain, photophobia and burning and to improve the patient’s visual acuity. This assessment was the work of the Committee for Advanced Therapies (CAT). The approved indication for Holoclar is: “Treatment of adult patients with moderate to severe limbal stem cell deficiency (defined by the presence of superficial corneal neovascularisation in at least two corneal quadrants, with central corneal involvement, and severely impaired visual acuity), unilateral or bilateral, due to physical or chemical ocular burns. A minimum of 1-2 square millimeters of undamaged limbus is required for biopsy.” CAT and CHMP considered that Holoclar provided a first treatment option for LSCD and recommended a conditional marketing authorization. The authorization is conditional because the clinical data available for Holoclar is based on studies that are ongoing as treated patients are watched after their eye surgery. This the data collection is not yet comprehensive, and additional study on the use of Holoclar needs to be conducted.
The opinion adopted by the CHMP at its December 2014 meeting is an intermediary step on Holoclar’s path to patient access. The CHMP opinion will now be sent to the European Commission for a decision on an EU-wide marketing authorization.
Embryonic stem cells are derived from human embryos, can only grow in culture indefinitely, and have the ability to potentially differentiate into any adult cell type in the human body. Because cell and tissues made from embryonic stem cells bear the same tissue types as the embryos from which they were derived, they will be rejected by the immune system patient. However, there are sites in our bodies were the immune system does not go, and that includes the central nervous system and the eyes. This is the reason why clinical trials with embryonic stem cell-derived cells have focused, to date, on spinal cord injuries and eye diseases.
Several clinical trials have examined the ability of retinal pigmented epithelial (RPE) cells made from embryonic stem cells to treat patients with dry macular degeneration or an inherited eye disease called Stargardt’s disease. Data from these trials has been reported in an article in the medical journal The Lancet, and accordingly, none of the treated patients showed tumor formation or immunological rejection of the implants and, most impressively perhaps, partial blindness was reversed in about half of the eyes that received transplants.
The results might re-energize the quest to harness embryonic stem cells for human medicine. Dr. Anthony Atala of the Wake Forest Institute for Regenerative Medicine called the work “a major accomplishment” in an accompanying commentary on the article.
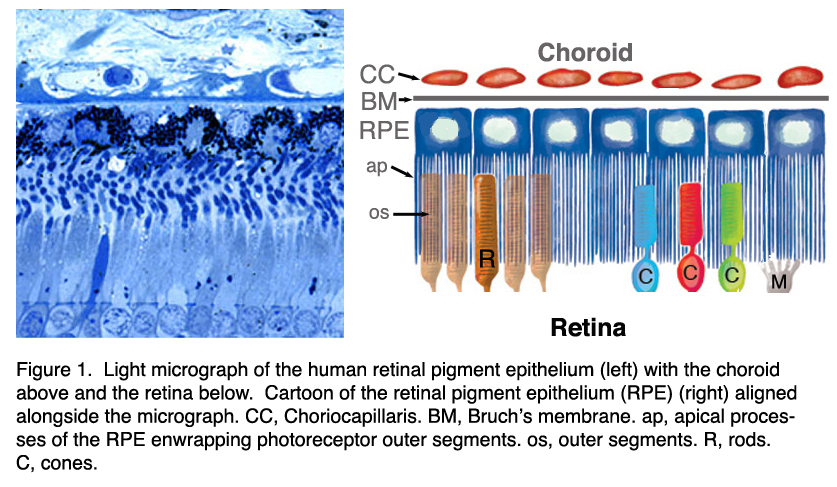
RPE cells lie just behind the photoreceptor cells in the retina of our eyes. Photoreceptors have their ends hurried in the RPE layer. This arrangement exists for a very good reason; the photoreceptors are exposed to high intensities of light and they suffer respectable amounts of oxidative damage. The components of the photoreceptors cells are made in the very lowest parts of the RPEs and then are eventually pushed to the ends of the cells. At the end of the photoreceptor cells, the RPEs relieve the photoreceptors of their photodamaged parts and gobble them down, and recycle the cellular components. Thus, RPE cells serve a photoreceptor cell repair and service cells. If the RPE cells begin to die, the photoreceptors are not long the this work either.
In the case of dry macular degeneration, which accounts for 90 percent of diagnosed cases of macular degeneration, the light-sensitive photoreceptor cells of the macula (the portion of the retina were the day vision is the sharpest) slowly break down. Damage to the macula causes blurring or spotty loss of central vision and yellowish cellular deposits called drusen (extracellular waste products from metabolism) form under the retina between the retinal pigmented epithelium (RPE) layer and a basement membrane called Bruch’s membrane, that supports the retina. An increase in the size and number of drusen is associated with the death of RPE and, consequently, photoreceptor cells, and is sometimes the first sign of dry macular degeneration.
Mutations in several genes have been identified in families with dry macular degeneration that increase the risk for dry macular degeneration. These include the SERPING1 gene, those genes that encode the complement system proteins factor H (CFH), factor B (CFB) and factor 3, and fibulin-5. Additionally, some environmental and behavioral factors also influence the risk a person will develop macular degeneration. These include smoking, exposure to blue light, ingestion of a high-fat diet, elevated blood pressure and serum cholesterol levels, and low vitamin D levels.
Stargardt’s disease is an inherited, juvenile form of macular degeneration that is caused by mutations in the ABCR gene. The protein encoded by this gene is a waste metabolite transporter, and defects in this protein cause the build up of a toxic metabolite called lipofuscin in the RPE cells, which leads to their demise and the death of the photoreceptors.
In this study, the main goal was to assess the safety of the transplanted cells. The study “provides the first evidence, in humans with any disease, of the long-term safety and possible biologic activity” of cells derived from embryos, said co-author Dr. Robert Lanza, chief scientific officer of Advanced Cell Technology, which produced the cells and funded the study.
Nine patients with Stargardt’s disease and nine with dry age-related macular degeneration received implants of the retinal cells in one eye. The other eye served as a control. Four eyes developed cataracts and two became inflamed, probably due to the patients’ age (median: 77) or the use of immune-supressing transplant drugs.
The implanted RPE cells survived in all 18 patients, most of whose vision improved. In those with macular degeneration, treated eyes saw a median of 14 additional letters on a standard eye chart a year after receiving the cells, with one patient gaining 19 letters. The untreated eyes got worse, overall. The Stargardt’s patients had similar results.
In real-life terms, patients who couldn’t see objects under 12 feet (4 meters) tall can now see normal-size adults.
The vision of one 75-year old rancher who was blind in the treated eye (20/400) improved to 20/40, enough to ride horses again, Lanza said. Others became able to use computers, read watches, go to the mall or travel to the airport alone for the first time in years.
While calling the results “encouraging,” stem cell expert Dusko Ilic of Kings College London, who was not involved in the work, warned that even if the larger clinical trial planned for later this year is also successful, “it will take years before the treatment becomes available.”
Other cell types can also form RPE cells and these include induced pluripotent stem cells, mesenchymal stem cells from fat (Ophthalmic Res. 2012;48 Suppl 1:1-5), adult retinal stem cells (Pigment Cell Melanoma Res. 2011 Feb;24(1):233-40), and iris pigmented epithelial cells (Prog Retin Eye Res. 2007 May;26(3):302-21). We do not need to destroy embryos to treat eye diseases with stem cells.
Nearly 10% of all Americans suffer from Dry eye syndrome (DES), which makes this disorder one of the most common ocular diseases. Most of the currently-available treatments are palliative, but few therapeutic agents target the biological causes of DES. Many factors contribute to DES, but one of the most important factors in the cause of DES is inflammation of the ocular surface.
Since mesenchymal stem cells (MSCs) have been shown to suppress inflammation, using MSCs to treat DES seems to be a viable treatment option. MSCs can also repair tissues by regulating excessive immune responses in various diseases.
Thus Joo Youn Oh from the Seoul National University in Seoul, Korea and his colleagues investigated the therapeutic potential of MSCs in a mouse model of an inflammation-mediated dry eye. They induced DES in these mice by injecting a plant protein into the eye that grabs sugars into the eye. This protein injection dries out the eyes in these mice and induces a kind of DES-like condition.
Then they found that the administration of MSCs into the eye reduced the infiltration of immune cells into the eye and overall decreased eye inflammation. Administration of MSCs into the eye also significantly increased tear production and also increased the number of conjunctival goblet cells, which secrete lubricating mucus so that the eye lid slides gently over the eye surface. Further investigation showed that the structural integrity of the eye surface, known as the cornea, was well-preserved by MSCs.
When taken together, ocular administration of MSCs seem to suppress the inflammation that either accompanies or contributes to DES. These results also suggest that MSCs may provide a potential therapy for those diseases that cause inflammation of the ocular surface and adversely affect the eye because of it.
Johns Hopkins University medical researchers have reported the derivation of human induced-pluripotent stem cells (iPSCs) that can repair damaged retinal vascular tissue in mice. These stem cells, which were derived from human umbilical cord-blood cells and reprogrammed into an embryonic-like state, were derived without the conventional use of viruses, which can damage genes and initiate cancers. This safer method of growing the cells has drawn increased support among scientists, they say, and paves the way for a stem cell bank of cord-blood derived iPSCs to advance regenerative medical research.
In a report published Jan. 20 in the journal Circulation, Johns Hopkins University stem cell biologist Elias Zambidis and his colleagues described laboratory experiments with these non-viral, human retinal iPSCs, that were created generated using the virus-free method Zambidis first reported in 2011.
“We began with stem cells taken from cord-blood, which have fewer acquired mutations and little, if any, epigenetic memory, which cells accumulate as time goes on,” says Zambidis, associate professor of oncology and pediatrics at the Johns Hopkins Institute for Cell Engineering and the Kimmel Cancer Center. The scientists converted these cells to a status last experienced when they were part of six-day-old embryos.
Instead of using viruses to deliver a gene package to the cells to turn on processes that convert the cells back to stem cell states, Zambidis and his team used plasmids, which are rings of DNA that replicate briefly inside cells and then are degraded and disappear.
Next, the scientists identified and isolated high-quality, multipotent, vascular stem cells that resulted from the differentiation of these iPSC that can differentiate into the types of blood vessel-rich tissues that can repair retinas and other human tissues as well. They identified these cells by looking for cell surface proteins called CD31 and CD146. Zambidis says that they were able to create twice as many well-functioning vascular stem cells as compared with iPSCs made with other methods, and, “more importantly these cells engrafted and integrated into functioning blood vessels in damaged mouse retina.”
Working with Gerard Lutty, Ph.D., and his team at Johns Hopkins’ Wilmer Eye Institute, Zambidis’ team injected these newly iPSC-derived vascular progenitors into mice with damaged retinas (the light-sensitive part of the eyeball). The cells were injected into the eye, the sinus cavity near the eye or into a tail vein. When Zamdibis and his colleagues took images of the mouse retinas, they found that the iPSC-derived vascular progenitors, regardless of injection location, engrafted and repaired blood vessel structures in the retina.
“The blood vessels enlarged like a balloon in each of the locations where the iPSCs engrafted,” says Zambidis. Their vascular progenitors made from cord blood-derived iPSCs compared very well with the ability of vascular progenitors derived from fibroblast-derived iPSCs to repair retinal damage.
Zambidis says that he has plans to conduct additional experiments in diabetic rats, whose conditions more closely resemble human vascular damage to the retina than the mouse model used for the current study, he says.
With mounting requests from other laboratories, Zambidis says he frequently shares his cord blood-derived iPSC with other scientists. “The popular belief that iPSCs therapies need to be specific to individual patients may not be the case,” says Zambidis. He points to recent success of partially matched bone marrow transplants in humans, shown to be as effective as fully matched transplants.
“Support is growing for building a large bank of iPSCs that scientists around the world can access,” says Zambidis, although large resources and intense quality-control would be needed for such a feat. However, Japanese scientists led by stem-cell pioneer Shinya Yamanaka are doing exactly that, he says, creating a bank of stem cells derived from cord-blood samples from Japanese blood banks.
More than 8 million people worldwide suffer from corneal blindness; a form of blindness that results from cloudiness of the outermost covering of the eye, the cornea.
Usually, the cornea copes quite well with minor injuries or scrapes and scratches. If the cornea is scratched, healthy cells slide over quickly and patch the injury before infection occurs and vision is not adversely affected. However, if the scratch penetrates the cornea more deeply, then the healing process takes longer and can result in greater pain, blurred vision, tearing, redness, and extreme sensitivity to light. Such scratches may require professional treatment. Even deeper scratches can also cause corneal scarring, which results in a haze on the cornea that can greatly impair vision, and the patient might require a corneal transplant.
Alternatively, corneal stem cells can help heal a damaged cornea; especially in those cases where the cornea has been damaged to the point where the native stem cell population has suffered irreparable damage (e.g., chemical burns, eye infections, or cases where the patient was born with a corneal stem cell deficiency).
A feasible treatment for such cases is a corneal stem cell transplant from another eye or from cultured corneal stem cells. Unfortunately, this procedure has not yet been standardized to date.
Fortunately, researchers at the Eye Program at the Cedar-Sinai Regenerative Medicine Institute have designed a fast, new procedure for preparing human amniotic membrane to use as a scaffold for corneal stem cells. The membrane provides a foundation that supports the growth of stem cells that can be grafted onto the cornea.
To date, a standardized method does not exist for the preparation of amniotic membranes for culturing corneal stem cells. Many methods use chemicals and may leave behind amniotic cells and membrane components.
This new procedure, however, takes less than one minute and ensures complete amniotic cell removal and preservation of amniotic membrane components, and, as an added bonus, supports the overall growth of various stem and tissue cells.
“We believe that this straightforward and relatively fast procedure would allow easier standardization of amniotic membrane as a valuable stem cell support and improve the current standard of care in corneal stem cell transplantation,” said the lead author of this work Alexander Ljubimov, the director of the Eye Program at the Cedar-Sinai Regenerative Medicine Institute. “This new method may provide a better method for researchers, transplant corneal surgeons, and manufacturing companies alike.”
The amniotic membrane has several beneficial properties for corneal stem cells culturing and use in corneal transplantations. For this reason it is an attractive framework for the growth and culture of corneal stem cells and for corneal transplantations.
The new method for amniotic membrane preparation will provide a fast way to create scaffolds for cell expansion and might potentially streamline clinical applications of cell therapies.
Japanese researchers from Gifu Pharmaceutical University and Gifu University have reported that a type of protein found in stem cells taken from adipose (fat) tissue can reverse and prevent age-related, light-induced retinal damage in mice. These results may lead to treatments for patients faced with permanent vision loss.
According to the work done by these two research teams led by Drs. Hideaki Hara and Kazuhiro Tsuruma, a single injection of fat-derived stem cells (ASCs) reduced the retinal damage induced by light exposure in mice. This study also discovered that when fat-derived stem cells were grown in culture with retinal cells, the stem cells prevented the retinal cells from suffering damage after exposure to hydrogen peroxide and visible light both in the culture and in the retinas of live mice.
Additionally, Hara and Tsuruma and their colleagues discovered a protein in fat-derived stem cells called “progranulin.” This protein, progranulin, seems to play a central role in protecting other cells from suffering light-induced eye damage.
In the retina, which lies at the back of the eye, excessive light exposure causes degeneration of the photoreceptor cells that respond to light. Several studies have suggested that a long-term history of exposure to light might be an important factor in the onset of age-related macular degeneration. Photoreceptor loss is the primary cause of blindness in particular eye-specific degenerative diseases such as age-related macular degeneration and retinitis pigmentosa.
“However, there are few effective therapeutic strategies for these diseases,” Hideaki Hara, Ph.D., R.Ph., and Kazuhiro Tsuruma, Ph.D., R.Ph.
“Recent studies have demonstrated that bone marrow-derived stem cells protect against central nervous system degeneration with limited results. Just like the bone marrow stem cells, ASCs also self-renew and have the ability to change, or differentiate, as they grow. But since they come from fat, they can be obtained more easily under local anesthesia and in large quantities.”
The fat tissue used in the study was taken from mice and processed in the laboratory to isolate the fat-based stem cells. Afterwards, those cells were tested with cultured mouse retinal cells, and they show a robust protective effect. These successes suggested to the team to test their theory on a live group of mice that had retinal damage after exposure to intense levels of light.
Five days after receiving injections of the fat-based stem cells, the animals were tested for photoreceptor degeneration and retinal dysfunction. The results showed the degeneration had been significantly inhibited.
“Progranulin was identified as a major secreted protein of ASCs, which showed protective effects against retinal damage in culture and in animal tests using mice,” Drs. Hara and Tsuruma said. “As such, it may be a potential target for the treatment of degenerative diseases of the retina such as age-related macular degeneration and retinitis pigmentosa. The ASCs reduced photoreceptor degeneration without engraftment, which is concordant with the results of previous studies using bone marrow stem cells.”
“This study, suggesting that the protein progranulin may play a pivotal role in protecting against retinal light-induced damage, points to the potential for new therapeutic approaches to degenerative diseases of the retina,” said, Anthony Atala, MD, editor of STEM CELLS Translational Medicine and director of the Wake Forest Institute for Regenerative Medicine, where this work was published.
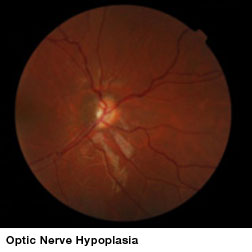
Optic nerve hypoplasia (ONH), an underdevelopment of optic nerves that occurs during fetal development, can appear as an isolated condition or as a part of a group of disorders characterized by brain anomalies, developmental delay, and endocrine abnormalities. ONH is a leading cause of blindness in children in North America and Europe and is the only cause of childhood blindness that shows increasing prevalence. No treatments have been shown to improve vision in these children.
Because stem cells heal or even regenerate some tissues, some have considered stem cell treatments as an option for this condition. However, a very small clinical study at Children’s Hospital Los Angeles found no evidence that stem cell therapies improve vision for children with optic nerve hypoplasia (ONH). Their results are reported in the Journal of the American Association for Pediatric Ophthalmology and Strabismus (AAPOS).
Families with a child that has ONH are traveling to China to undergo stem cell treatments that would be illegal in the United States. Because there are presently no viable treatment options available to improve vision in ONH children, such trips are often an act of desperation. The American Association for Pediatric Ophthalmology and Strabismus has also expressed its concern about these procedures, which are usually rather expensive, and have a dubious safety record.
Pediatric neuro-ophthalmologist Mark Borchert, MD, director of both the Eye Birth Defects and Eye Technology Institutes in The Vision Center at Children’s Hospital Los Angeles, realized that a controlled trial of sufficient size was needed to evaluate whether stem cell therapy is effective as a treatment for children with ONH. He agreed to conduct an independent study at the behest of Beike Biotech, which is based in Shenzhen, China and offers a stem cell treatment for ONH. This treatment uses donor umbilical cord stem cells and injects these cells into the cerebrospinal fluid.
Beike Biotech identified 10 children with bilateral ONH (ages 7 to 17 years) who had volunteered to travel to China for stem cell therapy. These patients gave their consent to participate in the study and Children’s Hospital found matched controls from their clinic. However, only two case-controlled pairs were evaluated because Beike Biotech was only able to recruit two patients.
Treatments consisted of six infusions over a 16-day period of umbilical cord-derived mesenchymal stem cells and daily infusions of growth factors. Visual acuity, optic nerve size, and sensitivity to light were to be evaluated one month before stem cell therapy and three and nine months after treatment.
Unfortunately no therapeutic effect was found in the two case-control pairs that were enrolled. “The results of this study show that children greater than 7 years of age with ONH may have spontaneous improvement in vision from one examination to the next. This improvement occurs equally in children regardless of whether or not they received treatment. Other aspects of the eye examination included pupil responses to light and optic nerve size; these did not change following treatment. The results of this research do not support the use of stem cells in the treatment of ONH at this time,” said lead author Cassandra Fink, MPH, program administrator at The Vision Center, Children’s Hospital Los Angeles.
However, confounding factors affect the interpretation of these results because the test subjects received additional alternative therapies (acupuncture, functional electrical stimulation and exercise) while receiving stem cell treatments. They were not supposed to receive such treatments. Additionally, the investigators could not determine the effect of these additional therapies on the subjects’ eyes.
“This study underscores the importance of scientifically testing these procedures to validate them and ensure their safety. Parents of afflicted children should be aware that the science behind the use of stem cell technology is unclear. This study takes a step toward testing this technology and finds no beneficial effect,” said William V. Good, MD, senior associate editor, Journal of AAPOS and Clinical Professor of Ophthalmology and Senior Scientist at the Smith-Kettlewell Eye Research Institute.
Basically, we have an incredibly small study that is also poorly controlled. Because the optic nerve forms during embryonic, fetal and postnatal development, using stem cells to make new nerves seems like a long shot as a treatment. I better treatment strategy might be to increase the myelination of the optic nerve with neural stem cells, oligodendrocyte precursor cells (OPCs), or Schwann cells. In general, this study does little to establish the lack of efficacy of such a stem cell treatment.
The first clinical trial that utilizes induced pluripotent stem cells has been given a green light. For this clinical trial six patients who suffer from age-related macular degeneration will donate skin biopsies and the cells from these skin biopsies will be used to generate induced pluripotent stem (iPS) cells in the laboratory. After those iPS cell lines are screened for safety (normal numbers of chromosomes, no mutations in critical genes, etc.), they will be differentiated into retinal cells. The retinal cells will be transplanted into the retinas of these six patients.
This clinical trial was approved by Japan Health Minister Norihisa Tamura and it will be next summer by Masayo Takahashi. Dr. Takahashi is a retinal regeneration expert and a colleague of the man who first developed iPS cells, Shinya Yamanaka. Yamanaka won the Nobel Prize for his discovery of iPSCs last year. In fact, this clinical trial epitomizes, in the eyes of many, the determination of Japanese scientists and politicians to dominate the iPS cell field. This national ambition kicked into high gear after Yamanaka shared the Nobel Prize for Physiology or Medicine last October for his iPS cell work.
Norihisa Tamura, Japanese Minister of HealthMasayo Takahashi, MD, PhD, Riken Center for Developmental Biology.
“If things continue this way, this will be the first in-clinic study in iPS cell technology,” says Doug Sipp of the Riken Center for Developmental Biology (CDB). The CDB, Takahashi’s institute, will co-run the trial with Kobe’s Institute for Biomedical Research and Innovation. “It’s exciting.”
Sipp, however, also noted that this move has not surprised anyone in Japan, since the Japanese stem cell community has heavily invested in iPS cells. Nevertheless, since Takahashi yet to formally publish the details of her trial, some have questioned whether she is actually ready to move forward. IPS cells are viewed as the perfect compromise for regenerative medicine. They are adult, and therefore do not require the destruction of human embryos for their establishment, and they are also pluripotent like an embryonic cell, which makes them relatively powerful sources for regenerative medicine.
Critics, however, warn that iPS cells were only discovered in 2007. To date, they remain difficult to create and culture and they can become tumorous in many hands. However, many labs have a great deal of expertise and skill when it comes to handling and deriving iPS cells. These labs derive and culture iPS cells routinely. In fact, Sipp notes that Riken’s CDB alone has produced world-class work with all kinds of stem cells, including embryonic stem (ES) cells, which are the models for iPS cells.
Additionally, Sipp and others point out that a scientist who has collaborated with Takahashi in the past, Riken’s Yoshiki Sasai, is doing groundbreaking work with ES cells and the eye. The British journal Nature has called Sasai “The Brainmaker,” and has said that his research is “wowing” the world.
The Japanese government has also soundly funded Takahashi’s trail. The health ministry’s recent stimulus plan set aside more money for stem cells (in particular iPS cells) than anything else. According to the journal Nature, the Japanese government sequestered 21.4 billion yen ($215 million) for stem cell research. Of this pot of money, the health ministry provided 700 million yen ($7 million) for a cell-processing center to support Takahashi before her trial was even approved. Two centers devoted to iPS cells are slated to be built with 2.2 billion yen ($22 million). The AFP reports the prime minister has set aside a breathtaking $1.18 billion, for iPS-cell work. Yamanaka has told Nature that the Japanese government seems to be “telling us to rush iPS cell-related technologies to patients as quickly as possible.”
Robert Lanza, CSO of Advanced Cell Technology, might once have been the logical bet to be first to the clinic with iPS cells. Unlike Takahashi, he has three ES cell trials under his belt, and has started talks with the FDA about transplanting iPS cell-derived platelets, but his iPS proposal is taking longer. Lanza bitterly noted, not without justification, “We don’t have the prime minister and emperor to speed things along for us.”
Since 2007, the year that Yamanaka reported the derivation of iPS cells from adult cells, Japan has focused on iPS cells. Yamanaka showed that increasing the expression of four genes could change limited adult human cells into potent, embryonic-like cells. “At Yamanaka’s institute alone, there are at least 20 teams focusing on iPS cells now,” Sipp says. There are teams at Riken, the Universities of Tokyo and Keio, and others. “A lot is happening here.” In fact, the Center for IPS Cell Research and Application was created expressly for Yamanaka.
Takahashi has reported part of the design of her clinical trial at scientific meetings. She told the International Society for Stem Cell Research in June 2012 she had created iPS-cell derived retinal pigment epithelial (RPE) cells for transplantation. RPE cells lie behind the photoreceptors in the retina, and the photoreceptors have their ends embedded into the RPE. The RPE cells replenish and nourish the photoreceptors, and without the RPE cells, the photoreceptors die from the damage incurred by exposure to light.
Death of the RPE cells cause eventual death of photoreceptors and that results in blindness. At the International Society for Stem Cell Research conference, Takahashi reported her that her iPS cell-derived RPEs possess proper structure and gene expression. They also do not produce tumors when transplanted into mice, and survive at least six months when transplanted into the retinas of monkeys. The vision of these animals, however, was not tested. She did note that some AMD patients’ sight improves when RPE cells are moved from the eye’s periphery to its center.
Retinal pigment epithelial cells derived from iPS cells.
Takahashi has published many iPS and ES cell papers. These papers include two papers with Yamanaka: one on creating retinal cells from iPS cells, and one on creating safe iPS cells. However she has not published trial details, which is not required, but such a landmark trial should be transparent, as argued by many stem cell experts.
Still, according to Sipp, Takahashi has submitted a relevant paper to a top journal for review, which shows that this clinical trial is purely a determination of the safety of the procedure. Lanza has reported his trials in the journal The Lancet, and similar, but small, trials are doing well. His three ES cell trials treated Stargardt’s macular dystrophy and Age-related Macular Degeneration. Lanza’s trial, however, treated “dry” macular degeneration, while Takahashi’s trial will treat “wet” Age-related Macular Degeneration, which is good news for Takahashi.
Paul Knoepfler, a UC Davis stem cell scientist who runs a widely read blog site, has written that the ministry overseeing Takahashi’s trial will reportedly monitor some key factors: gene sequencing and tumorigenicity. But Knoepfler, like others, would like to see more details.
The Japanese Health Ministry and the US FDA recently agreed to devise a joint regulatory framework for retinal iPS cell clinical trials, which will come on line 2015. Takahashi’s trial is set for 2014.

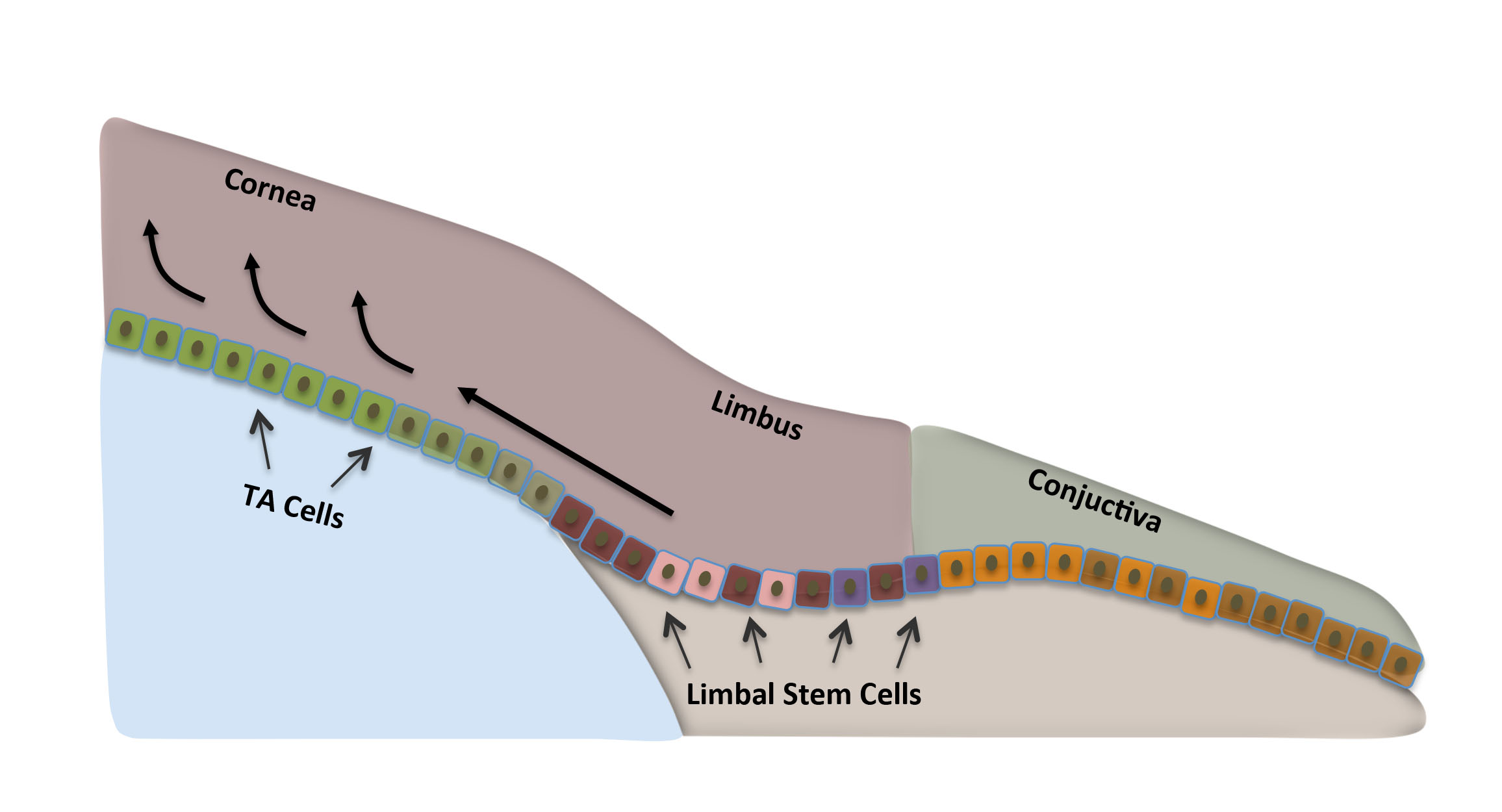
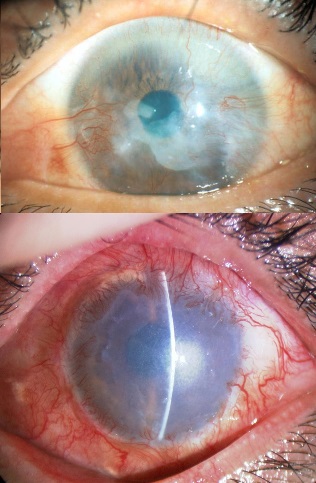
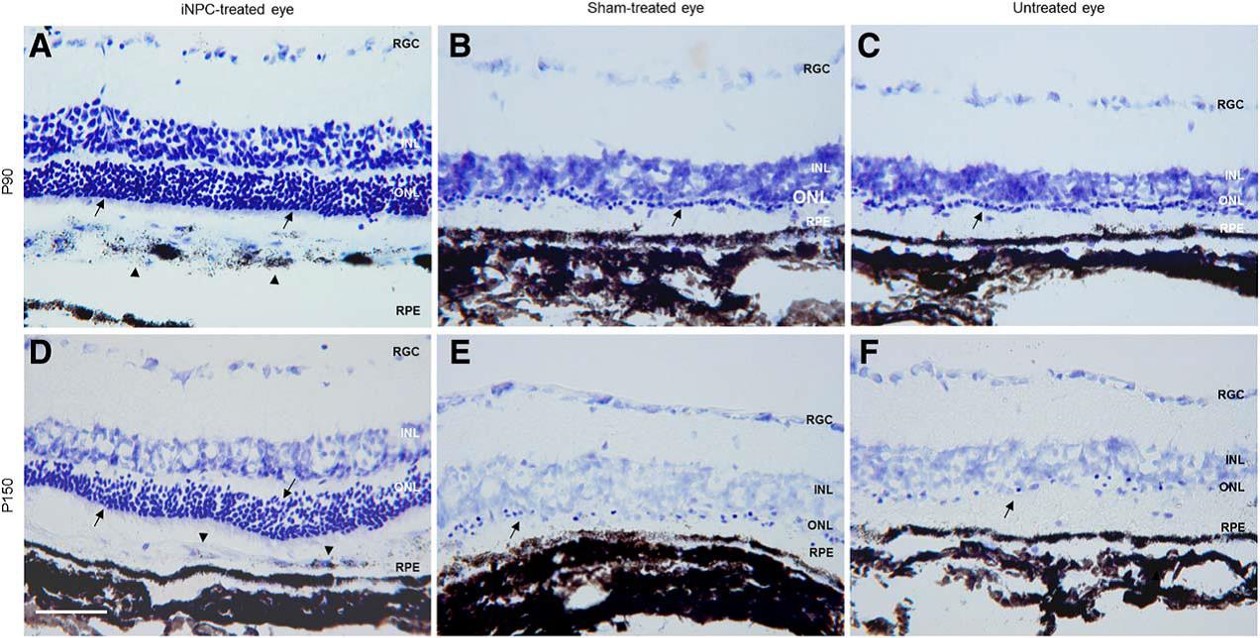
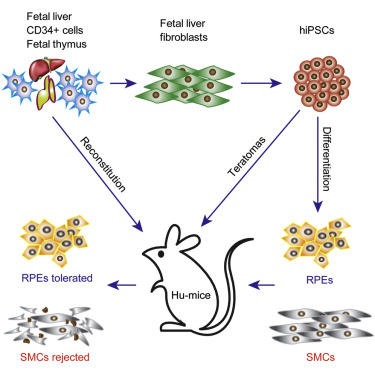
![Structures of opsins and of the chromophore retinal. (a) A model of the secondary structure of bovine rhodopsin. Amino-acid residues that are highly conserved in the whole opsin family are shown with a gray background. The retinal-binding site (K296) and the counterion position (E113) are marked with bold circles, as is E181, the counterion in opsins other than the vertebrate visual and non-visual ones. C110 and C187 form a disulfide bond. (b) The chemical structures of the 11-cis and all-trans forms of retinal. (c) The crystal structure of bovine rhodopsin (Protein DataBank ID: 1U19 [PDB:1U19]). The chromophore 11-cis-retinal, K296 and E113 are shown in stick representation in the ringed area. (d) The structure of the Schiff base linkage formed by retinal within the bovine opsin, together with the counterion that stabilizes it.](https://beyondthedish.wordpress.com/wp-content/uploads/2015/08/opsins.jpg)